› Forums › General Melanoma Community › Acquired resistance to BRAF inhibitors
- This topic has 66 replies, 5 voices, and was last updated 13 years, 11 months ago by
Harry in Fair Oaks.
- Post
-
- October 10, 2011 at 4:58 pm
So before you try PLX4032 (ZELBORAF/Verurafenib) as one of your trials if you are BRAF+, You may want to look into a BRAF + MEK trials first.
"Acquired resistance to BRAF inhibitors mediated by a RAF kinase switch in melanoma can be overcome by cotargeting MEK and IGF-1R/PI3K" -Dr. Meenhard Herlyn
There is also some new out about BRAF inhibitors + Metformin.
Best regards
Jimmy B
So before you try PLX4032 (ZELBORAF/Verurafenib) as one of your trials if you are BRAF+, You may want to look into a BRAF + MEK trials first.
"Acquired resistance to BRAF inhibitors mediated by a RAF kinase switch in melanoma can be overcome by cotargeting MEK and IGF-1R/PI3K" -Dr. Meenhard Herlyn
There is also some new out about BRAF inhibitors + Metformin.
Best regards
Jimmy B
- Replies
-
-
- October 10, 2011 at 7:18 pm
Hi Everyone,
For what it is worth, I met with my onc (melanoma specialist ) to discuss getting into to the Braf/Mek trial. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has going for awhile now. He has also been involved with Braf trials for many years. He said that it is only a matter of time for Braf/Mek to stop working like Braf alone. It still is not the magic bullet.
He also told me by taking Braf and/or Mek that once an inhibitor drug (like Braf and Mek) stopped working that my tumors would have been altered by the inhibitor drug which would make my tumors more resistant to an immunology drug like yervoy & PD1.
-
- October 10, 2011 at 7:18 pm
Hi Everyone,
For what it is worth, I met with my onc (melanoma specialist ) to discuss getting into to the Braf/Mek trial. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has going for awhile now. He has also been involved with Braf trials for many years. He said that it is only a matter of time for Braf/Mek to stop working like Braf alone. It still is not the magic bullet.
He also told me by taking Braf and/or Mek that once an inhibitor drug (like Braf and Mek) stopped working that my tumors would have been altered by the inhibitor drug which would make my tumors more resistant to an immunology drug like yervoy & PD1.
-
- October 10, 2011 at 8:49 pm
Treating Melanoma: One Drug is Good, Two May Be Safer
Treating patients with advanced melanoma whose tumors have BRAF mutations with a BRAF inhibitor plus another targeted therapy appears to be at least as effective as using the BRAF inhibitor alone, and the combined therapy substantially reduces some of the side effects of each agent used alone, researchers reported at the ASCO annual meeting.
The findings come from a phase I clinical trial in which patients systematically received escalating doses of the experimental BRAF-targeted agent, GSK436, and a different experimental agent, GSK212, that targets a protein called MEK, which is in the same molecular signaling pathway as BRAF.
In earlier phase I trials, both drugs produced strong tumor responses in patients with advanced melanoma with BRAF mutations, but both had toxicities, including the development of squamous cell carcinomas in patients treated with GSK436 and an acne-like rash in patients treated with GSK212.
Among the 109 patients in the trial who have received both drugs together, only one developed a squamous cell carcinoma and the incidence of skin rashes was substantially reduced, reported Dr. Jeffrey Infante of the Sarah Cannon Research Institute in Nashville, TN. Only rarely did the dose of the drugs have to be reduced because of side effects, he added.
Of the 71 patients in the trial who had not yet been treated with a BRAF inhibitor, Dr. Infante said, between 55 and 77 percent had stable disease or some tumor shrinkage—including five patients who had complete responses—after receiving both drugs simultaneously, depending on the dose of the drugs used.
"The addition of a MEK inhibitor is clearly one of the logical next steps to improve upon the efficacy of single-agent BRAF inhibitors," he said.
-
- October 10, 2011 at 8:49 pm
Treating Melanoma: One Drug is Good, Two May Be Safer
Treating patients with advanced melanoma whose tumors have BRAF mutations with a BRAF inhibitor plus another targeted therapy appears to be at least as effective as using the BRAF inhibitor alone, and the combined therapy substantially reduces some of the side effects of each agent used alone, researchers reported at the ASCO annual meeting.
The findings come from a phase I clinical trial in which patients systematically received escalating doses of the experimental BRAF-targeted agent, GSK436, and a different experimental agent, GSK212, that targets a protein called MEK, which is in the same molecular signaling pathway as BRAF.
In earlier phase I trials, both drugs produced strong tumor responses in patients with advanced melanoma with BRAF mutations, but both had toxicities, including the development of squamous cell carcinomas in patients treated with GSK436 and an acne-like rash in patients treated with GSK212.
Among the 109 patients in the trial who have received both drugs together, only one developed a squamous cell carcinoma and the incidence of skin rashes was substantially reduced, reported Dr. Jeffrey Infante of the Sarah Cannon Research Institute in Nashville, TN. Only rarely did the dose of the drugs have to be reduced because of side effects, he added.
Of the 71 patients in the trial who had not yet been treated with a BRAF inhibitor, Dr. Infante said, between 55 and 77 percent had stable disease or some tumor shrinkage—including five patients who had complete responses—after receiving both drugs simultaneously, depending on the dose of the drugs used.
"The addition of a MEK inhibitor is clearly one of the logical next steps to improve upon the efficacy of single-agent BRAF inhibitors," he said.
-
- October 11, 2011 at 5:06 am
I'm a participant in the GSK combo trial you are referring to. I get a daily dose of 300 mg of the BRAF inhibitor, and 2 mg a day of the MEK inhibitor (these are the max amounts of each drug in this study). I can vouch for the fact that the side-effects are minimal for this 2 drug combo.
As far as effectiveness and durabilty of response, I don't think anyone can make a final judgment yet – the trial has not run its course, and the results have not been evaluated. But anecdotally, I am approaching the 24th week, and the results are great so far. My sub-q's are gone, and all other mets are stable or shrinking.
I think that any statements about the BRAF and/or MEK drugs making tumors resistant to other therapies (such as Yervoy) are pure speculation. Where is the evidence? Just because a Dr. voices such an opinion does not make it so.
Best wishes,
Harry (so far an 11-year Stage IV survivor)
-
- October 11, 2011 at 5:06 am
I'm a participant in the GSK combo trial you are referring to. I get a daily dose of 300 mg of the BRAF inhibitor, and 2 mg a day of the MEK inhibitor (these are the max amounts of each drug in this study). I can vouch for the fact that the side-effects are minimal for this 2 drug combo.
As far as effectiveness and durabilty of response, I don't think anyone can make a final judgment yet – the trial has not run its course, and the results have not been evaluated. But anecdotally, I am approaching the 24th week, and the results are great so far. My sub-q's are gone, and all other mets are stable or shrinking.
I think that any statements about the BRAF and/or MEK drugs making tumors resistant to other therapies (such as Yervoy) are pure speculation. Where is the evidence? Just because a Dr. voices such an opinion does not make it so.
Best wishes,
Harry (so far an 11-year Stage IV survivor)
-
- October 11, 2011 at 5:06 am
I'm a participant in the GSK combo trial you are referring to. I get a daily dose of 300 mg of the BRAF inhibitor, and 2 mg a day of the MEK inhibitor (these are the max amounts of each drug in this study). I can vouch for the fact that the side-effects are minimal for this 2 drug combo.
As far as effectiveness and durabilty of response, I don't think anyone can make a final judgment yet – the trial has not run its course, and the results have not been evaluated. But anecdotally, I am approaching the 24th week, and the results are great so far. My sub-q's are gone, and all other mets are stable or shrinking.
I think that any statements about the BRAF and/or MEK drugs making tumors resistant to other therapies (such as Yervoy) are pure speculation. Where is the evidence? Just because a Dr. voices such an opinion does not make it so.
Best wishes,
Harry (so far an 11-year Stage IV survivor)
-
- October 10, 2011 at 8:49 pm
Treating Melanoma: One Drug is Good, Two May Be Safer
Treating patients with advanced melanoma whose tumors have BRAF mutations with a BRAF inhibitor plus another targeted therapy appears to be at least as effective as using the BRAF inhibitor alone, and the combined therapy substantially reduces some of the side effects of each agent used alone, researchers reported at the ASCO annual meeting.
The findings come from a phase I clinical trial in which patients systematically received escalating doses of the experimental BRAF-targeted agent, GSK436, and a different experimental agent, GSK212, that targets a protein called MEK, which is in the same molecular signaling pathway as BRAF.
In earlier phase I trials, both drugs produced strong tumor responses in patients with advanced melanoma with BRAF mutations, but both had toxicities, including the development of squamous cell carcinomas in patients treated with GSK436 and an acne-like rash in patients treated with GSK212.
Among the 109 patients in the trial who have received both drugs together, only one developed a squamous cell carcinoma and the incidence of skin rashes was substantially reduced, reported Dr. Jeffrey Infante of the Sarah Cannon Research Institute in Nashville, TN. Only rarely did the dose of the drugs have to be reduced because of side effects, he added.
Of the 71 patients in the trial who had not yet been treated with a BRAF inhibitor, Dr. Infante said, between 55 and 77 percent had stable disease or some tumor shrinkage—including five patients who had complete responses—after receiving both drugs simultaneously, depending on the dose of the drugs used.
"The addition of a MEK inhibitor is clearly one of the logical next steps to improve upon the efficacy of single-agent BRAF inhibitors," he said.
-
- October 11, 2011 at 5:17 am
Could you please ask your onc where people can get their hands on data showing that acquired resistance to BRAF/MEK drugs will make tumors more resistant to Yervoy and PD1? This is the first time I've heard of this.
Best wishes,
Harry (11-year Stage IV survivor, now on BRAF/MEK study)
-
- October 11, 2011 at 5:17 am
Could you please ask your onc where people can get their hands on data showing that acquired resistance to BRAF/MEK drugs will make tumors more resistant to Yervoy and PD1? This is the first time I've heard of this.
Best wishes,
Harry (11-year Stage IV survivor, now on BRAF/MEK study)
-
- October 11, 2011 at 4:59 pm
First heard for me too….. would like to see the evidence behind this assertion since BRAK, MEK and ipi target completely different pathways in melanoma tumorigenesis
Hawaii Bob, Stage IIA
-
- October 11, 2011 at 4:59 pm
First heard for me too….. would like to see the evidence behind this assertion since BRAK, MEK and ipi target completely different pathways in melanoma tumorigenesis
Hawaii Bob, Stage IIA
-
- October 11, 2011 at 4:59 pm
First heard for me too….. would like to see the evidence behind this assertion since BRAK, MEK and ipi target completely different pathways in melanoma tumorigenesis
Hawaii Bob, Stage IIA
-
- October 11, 2011 at 5:17 am
Could you please ask your onc where people can get their hands on data showing that acquired resistance to BRAF/MEK drugs will make tumors more resistant to Yervoy and PD1? This is the first time I've heard of this.
Best wishes,
Harry (11-year Stage IV survivor, now on BRAF/MEK study)
-
- October 10, 2011 at 7:18 pm
Hi Everyone,
For what it is worth, I met with my onc (melanoma specialist ) to discuss getting into to the Braf/Mek trial. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has going for awhile now. He has also been involved with Braf trials for many years. He said that it is only a matter of time for Braf/Mek to stop working like Braf alone. It still is not the magic bullet.
He also told me by taking Braf and/or Mek that once an inhibitor drug (like Braf and Mek) stopped working that my tumors would have been altered by the inhibitor drug which would make my tumors more resistant to an immunology drug like yervoy & PD1.
-
- October 12, 2011 at 1:23 pm
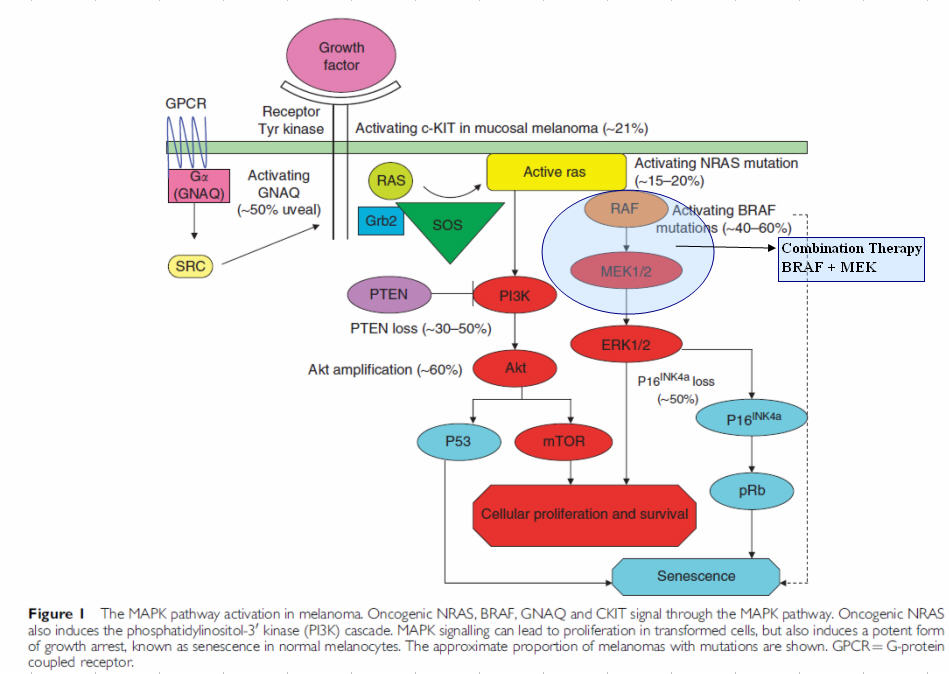
"Ultimately, the research suggested that a combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways represent the optimal combination for use with a BRAF inhibitor to mitigate the development of resistance. "
"All three compounds we used to overcome resistance to BRAF inhibition are already undergoing clinical evaluation. Therefore, we believe this particular combination approach represents a promising and translatable strategy for addressing BRAF inhibitor resistance in a subset of melanomas," Dr. Lo says.
"Among clinical trials currently enrolling melanoma patients with BRAF mutations are those combining BRAF and MEK inhibition and others combining PI3K/mTOR and MEK inhibition. Other highly-watched trials include those which combine a BRAF inhibitor with ipilimumab. "
Source: Dematology Times
-
- October 12, 2011 at 1:23 pm
"Ultimately, the research suggested that a combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways represent the optimal combination for use with a BRAF inhibitor to mitigate the development of resistance. "
"All three compounds we used to overcome resistance to BRAF inhibition are already undergoing clinical evaluation. Therefore, we believe this particular combination approach represents a promising and translatable strategy for addressing BRAF inhibitor resistance in a subset of melanomas," Dr. Lo says.
"Among clinical trials currently enrolling melanoma patients with BRAF mutations are those combining BRAF and MEK inhibition and others combining PI3K/mTOR and MEK inhibition. Other highly-watched trials include those which combine a BRAF inhibitor with ipilimumab. "
Source: Dematology Times
-
- October 12, 2011 at 3:47 pm
Jim,
Interesting that you should post the research done by Dr. Lo at UCLA. My Onc is Dr. Ribas at UCLA who has been doing the research studies with Dr. Lo. on Braf.
Long story short, I had an appt. with Dr. Ribas last week. Dr. Ribas told me, based on their most recent research, Dr. Lo & himself believe that even with combining Braf with "combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways" that tumors will still eventually become resistant to the Braf/combo drugs.It would only be a matter of time.
When discussing if I should do the Braf/Mek combo trial, he recommended that I do an immmnunolgy drug like IPI or a PD1 drug. Dr. Ribas told me based on their most recent research that when you take an inhibitor drug, somehow the inhibitor drug alters the tumor. Then when the Braf/combo eventually stops working, because the tumor has been altered and there is tumor progresses, Dr.Ribas says it is then more difficult for a person's immune system to kill the tumor cells.
Needless to say, it was disappointing to hear that the Braf/ combo drugs were not going to be the magic bullet.
For what it is worth, I am taking Dr.Ribas advice and doing an immmunology treatment.
-
- October 12, 2011 at 3:47 pm
Jim,
Interesting that you should post the research done by Dr. Lo at UCLA. My Onc is Dr. Ribas at UCLA who has been doing the research studies with Dr. Lo. on Braf.
Long story short, I had an appt. with Dr. Ribas last week. Dr. Ribas told me, based on their most recent research, Dr. Lo & himself believe that even with combining Braf with "combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways" that tumors will still eventually become resistant to the Braf/combo drugs.It would only be a matter of time.
When discussing if I should do the Braf/Mek combo trial, he recommended that I do an immmnunolgy drug like IPI or a PD1 drug. Dr. Ribas told me based on their most recent research that when you take an inhibitor drug, somehow the inhibitor drug alters the tumor. Then when the Braf/combo eventually stops working, because the tumor has been altered and there is tumor progresses, Dr.Ribas says it is then more difficult for a person's immune system to kill the tumor cells.
Needless to say, it was disappointing to hear that the Braf/ combo drugs were not going to be the magic bullet.
For what it is worth, I am taking Dr.Ribas advice and doing an immmunology treatment.
-
- October 12, 2011 at 4:41 pm
I guess if I was BRAF +, I would use the BRAF card only if my tumor burden was getting the critical stage where death of the host was aproaching. Knock down the # of tumors so, immunotherapy would have a fighting chance. Stop the therapy and add immunotherapy before the resistance takes place.
BRAF combo may be fine if you have low tumor burden. With a low burden, maybe the BRAF combo will be able to kill all the cells before the resistance begins. It's all a crap shoot.
-
- October 12, 2011 at 4:41 pm
I guess if I was BRAF +, I would use the BRAF card only if my tumor burden was getting the critical stage where death of the host was aproaching. Knock down the # of tumors so, immunotherapy would have a fighting chance. Stop the therapy and add immunotherapy before the resistance takes place.
BRAF combo may be fine if you have low tumor burden. With a low burden, maybe the BRAF combo will be able to kill all the cells before the resistance begins. It's all a crap shoot.
-
- October 12, 2011 at 4:41 pm
I guess if I was BRAF +, I would use the BRAF card only if my tumor burden was getting the critical stage where death of the host was aproaching. Knock down the # of tumors so, immunotherapy would have a fighting chance. Stop the therapy and add immunotherapy before the resistance takes place.
BRAF combo may be fine if you have low tumor burden. With a low burden, maybe the BRAF combo will be able to kill all the cells before the resistance begins. It's all a crap shoot.
-
- October 12, 2011 at 5:17 pm
Leaving aside the "magic bullet" issue (there probably will never be a "magic bullet," if what is meant is a single sure-fire cure for all melanoms), what does Dr. Ribas know that the scientists and study doctors carrying out the GSK BRAF/MEK trials don't yet know?
Those trials are ongoing Phase I or Phase II trials whose results will likely not be known for awhile. It may well be that the BRAF/MEK combo drugs will be found to confer only temporary improvement. That's to be determined one way or the other. In the absence of a "magic bullet," increased survival time is a good thing! IPI/Yervoy is not a permanent cure for most patients either (only IL-2 has been found to confer longterm survival – for the small fraction of patients that respond).
Best wishes,
Harry
-
- October 12, 2011 at 5:17 pm
Leaving aside the "magic bullet" issue (there probably will never be a "magic bullet," if what is meant is a single sure-fire cure for all melanoms), what does Dr. Ribas know that the scientists and study doctors carrying out the GSK BRAF/MEK trials don't yet know?
Those trials are ongoing Phase I or Phase II trials whose results will likely not be known for awhile. It may well be that the BRAF/MEK combo drugs will be found to confer only temporary improvement. That's to be determined one way or the other. In the absence of a "magic bullet," increased survival time is a good thing! IPI/Yervoy is not a permanent cure for most patients either (only IL-2 has been found to confer longterm survival – for the small fraction of patients that respond).
Best wishes,
Harry
-
- October 12, 2011 at 5:17 pm
Leaving aside the "magic bullet" issue (there probably will never be a "magic bullet," if what is meant is a single sure-fire cure for all melanoms), what does Dr. Ribas know that the scientists and study doctors carrying out the GSK BRAF/MEK trials don't yet know?
Those trials are ongoing Phase I or Phase II trials whose results will likely not be known for awhile. It may well be that the BRAF/MEK combo drugs will be found to confer only temporary improvement. That's to be determined one way or the other. In the absence of a "magic bullet," increased survival time is a good thing! IPI/Yervoy is not a permanent cure for most patients either (only IL-2 has been found to confer longterm survival – for the small fraction of patients that respond).
Best wishes,
Harry
-
- October 12, 2011 at 6:01 pm
Jim,
You are right. Dr. Ribas told me it was best to save"braf" card when I was in a situation that I needed it. Even at low burden, he stated, it was best NOT to alter the tumor with an inhibitor. I also had a consultant with Angeles Clinic & was told the same thing. Save Braf/mek combo drug and do an immunology treatment in hopes of a longer durable response.
Harry, you make a good point. I asked Dr. Ribas about Braf/Mek trial results thus far. Dr. Ribas told me he has has been doing the Braf/Mek trial at UCLA. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has doing for awhile now. Dr. Ribas did say these were his initial findings about Braf/mek combo. I think that he mentioned that the sponsor running the trial, are getting reports of some patients building a resistance to the combo drugs. However, Dr. Ribas did say the combo drug was less toxic which is a good thing.
I agree that if the braf/mek combo increases survival time like braf drug, it will help alot of people. I think the bottomline message I got from Dr. Ribas and Angles clinic is to do an immunology treatment first (no matter what your tumor burden is) Then do inhibitor drugs if immunology treatment does not work.
-
- October 12, 2011 at 6:01 pm
Jim,
You are right. Dr. Ribas told me it was best to save"braf" card when I was in a situation that I needed it. Even at low burden, he stated, it was best NOT to alter the tumor with an inhibitor. I also had a consultant with Angeles Clinic & was told the same thing. Save Braf/mek combo drug and do an immunology treatment in hopes of a longer durable response.
Harry, you make a good point. I asked Dr. Ribas about Braf/Mek trial results thus far. Dr. Ribas told me he has has been doing the Braf/Mek trial at UCLA. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has doing for awhile now. Dr. Ribas did say these were his initial findings about Braf/mek combo. I think that he mentioned that the sponsor running the trial, are getting reports of some patients building a resistance to the combo drugs. However, Dr. Ribas did say the combo drug was less toxic which is a good thing.
I agree that if the braf/mek combo increases survival time like braf drug, it will help alot of people. I think the bottomline message I got from Dr. Ribas and Angles clinic is to do an immunology treatment first (no matter what your tumor burden is) Then do inhibitor drugs if immunology treatment does not work.
-
- October 12, 2011 at 6:01 pm
Jim,
You are right. Dr. Ribas told me it was best to save"braf" card when I was in a situation that I needed it. Even at low burden, he stated, it was best NOT to alter the tumor with an inhibitor. I also had a consultant with Angeles Clinic & was told the same thing. Save Braf/mek combo drug and do an immunology treatment in hopes of a longer durable response.
Harry, you make a good point. I asked Dr. Ribas about Braf/Mek trial results thus far. Dr. Ribas told me he has has been doing the Braf/Mek trial at UCLA. He told me patients have already built up a resistance to the Braf/Mek drug in the trial that he has doing for awhile now. Dr. Ribas did say these were his initial findings about Braf/mek combo. I think that he mentioned that the sponsor running the trial, are getting reports of some patients building a resistance to the combo drugs. However, Dr. Ribas did say the combo drug was less toxic which is a good thing.
I agree that if the braf/mek combo increases survival time like braf drug, it will help alot of people. I think the bottomline message I got from Dr. Ribas and Angles clinic is to do an immunology treatment first (no matter what your tumor burden is) Then do inhibitor drugs if immunology treatment does not work.
-
- October 12, 2011 at 6:45 pm
I think that with the state of the science being what it is (and it is still rather cloudy) there are the expected differences of opinion among the experts. When I consulted with Dr. Steven O'Day in March of this year, presenting with sub-qs and bone tumors, he recommended the BRAF/MEK trial as his first choice. Then Yervoy (which had just been approved) if the BRAF/MEK did not work or quit working. FInally, if both those failed, IL-2 was seen by him as the "Hail Mary" option.
Best wishes,
Harry
-
- October 12, 2011 at 8:26 pm
I was told he is not practicing anywhere when I asked a couple of weeks ago.
Best wishes,
Harry
-
- October 12, 2011 at 8:26 pm
I was told he is not practicing anywhere when I asked a couple of weeks ago.
Best wishes,
Harry
-
- October 12, 2011 at 8:26 pm
I was told he is not practicing anywhere when I asked a couple of weeks ago.
Best wishes,
Harry
-
- October 12, 2011 at 6:45 pm
I think that with the state of the science being what it is (and it is still rather cloudy) there are the expected differences of opinion among the experts. When I consulted with Dr. Steven O'Day in March of this year, presenting with sub-qs and bone tumors, he recommended the BRAF/MEK trial as his first choice. Then Yervoy (which had just been approved) if the BRAF/MEK did not work or quit working. FInally, if both those failed, IL-2 was seen by him as the "Hail Mary" option.
Best wishes,
Harry
-
- October 12, 2011 at 6:45 pm
I think that with the state of the science being what it is (and it is still rather cloudy) there are the expected differences of opinion among the experts. When I consulted with Dr. Steven O'Day in March of this year, presenting with sub-qs and bone tumors, he recommended the BRAF/MEK trial as his first choice. Then Yervoy (which had just been approved) if the BRAF/MEK did not work or quit working. FInally, if both those failed, IL-2 was seen by him as the "Hail Mary" option.
Best wishes,
Harry
-
- October 12, 2011 at 6:03 pm
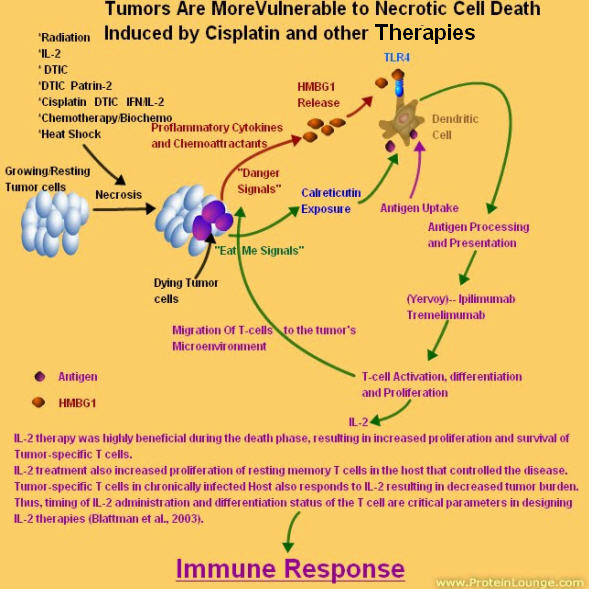
Harry, I thinks the "Magic Bullet" will be a combinatorial therapy. It will most likely drugs strung in a sequence that :
1) A drug combo to make the tumor more susceptible to Chemo to shed Tumor-Specific antigens from dying tumor cells (DTIC,Patrin-2,Cisplatin,TMZ,radiation,biochemo..etc)
2) a drug combo to suppress the Tregs and help activate T-cells (Yervoy,Anti-PD-1, Anti-Gal-3 ..etc)
3) Finally a drug that keeps the T-cell (Cytotoxic T-lymphocytes) activated, functional and that is needed for survival.
-
- October 12, 2011 at 6:55 pm
I really hope the "1-2-3" path you outline indeed leads to that holy grail, the "magic bullet." We must keep in mind the long, sometimes insurmountable, path between the theoretical and the eventual actual. But we can always hope – and be thankful for the advances of the last few years, even though they aren't all that we want.
Best wishes,
Harry
-
- October 12, 2011 at 7:18 pm
Harry, I want tell you, YOU have heard it here first.
I am living proof. From Stage IV to NED without surgery of 40 + Lung nodules in both lobes and sub Q's. Also there are others that had a simular regime, NED also. All the science is not worked out, but the theory is there. Sequence and Timing is the name of the game.
Warm regards,
Jimmy B
-
- October 12, 2011 at 7:18 pm
Harry, I want tell you, YOU have heard it here first.
I am living proof. From Stage IV to NED without surgery of 40 + Lung nodules in both lobes and sub Q's. Also there are others that had a simular regime, NED also. All the science is not worked out, but the theory is there. Sequence and Timing is the name of the game.
Warm regards,
Jimmy B
-
- October 12, 2011 at 8:13 pm
10-24-2005 when I was first diagnosed with melanoma
10-27-2005 I had a wide incision to remove the tumor off my back
3-6-2006, I started the High Dose Interferon treatment
7-10-2006, I started my clinical trial of Dicarbazine and Patrin
9-13-06(day 1)I had my first and only infusion of anti-CTLA-4 monoclonal antibodies 15mg/Kg
11-1-06, the first cycle of High dose Interleukin-2 (IL-2).
(day98) 12-19-06 we got the CT Scan Results: What a Christmas Present!!!!!! The tumors were shrinking!!!!!!!
-
- October 12, 2011 at 8:13 pm
10-24-2005 when I was first diagnosed with melanoma
10-27-2005 I had a wide incision to remove the tumor off my back
3-6-2006, I started the High Dose Interferon treatment
7-10-2006, I started my clinical trial of Dicarbazine and Patrin
9-13-06(day 1)I had my first and only infusion of anti-CTLA-4 monoclonal antibodies 15mg/Kg
11-1-06, the first cycle of High dose Interleukin-2 (IL-2).
(day98) 12-19-06 we got the CT Scan Results: What a Christmas Present!!!!!! The tumors were shrinking!!!!!!!
-
- October 12, 2011 at 8:13 pm
10-24-2005 when I was first diagnosed with melanoma
10-27-2005 I had a wide incision to remove the tumor off my back
3-6-2006, I started the High Dose Interferon treatment
7-10-2006, I started my clinical trial of Dicarbazine and Patrin
9-13-06(day 1)I had my first and only infusion of anti-CTLA-4 monoclonal antibodies 15mg/Kg
11-1-06, the first cycle of High dose Interleukin-2 (IL-2).
(day98) 12-19-06 we got the CT Scan Results: What a Christmas Present!!!!!! The tumors were shrinking!!!!!!!
-
- October 12, 2011 at 8:22 pm
Jim, I don't want to pick an argument with you – most of the treatments you champion are doubtlessly on the right path. But as elegantly as you present your information (and you have wonderful graphics), you are not living proof that your regimen is the "magic bullet." Nor are the other NED patients that you allude to. Your individual health outcome is anecdotal information, not scientific proof.
I have learned the hard way not to tempt the NED gods. After being almost 11 years NED after lung metastisis, I thought I was done with this thing. I even thought that the immunological trials I went through (vaccine and leukine) may have been the nails in the coffin. Imagine my surprise when the beast woke up and bit me this year!
Best wishes,
Harry
-
- October 12, 2011 at 8:22 pm
Jim, I don't want to pick an argument with you – most of the treatments you champion are doubtlessly on the right path. But as elegantly as you present your information (and you have wonderful graphics), you are not living proof that your regimen is the "magic bullet." Nor are the other NED patients that you allude to. Your individual health outcome is anecdotal information, not scientific proof.
I have learned the hard way not to tempt the NED gods. After being almost 11 years NED after lung metastisis, I thought I was done with this thing. I even thought that the immunological trials I went through (vaccine and leukine) may have been the nails in the coffin. Imagine my surprise when the beast woke up and bit me this year!
Best wishes,
Harry
-
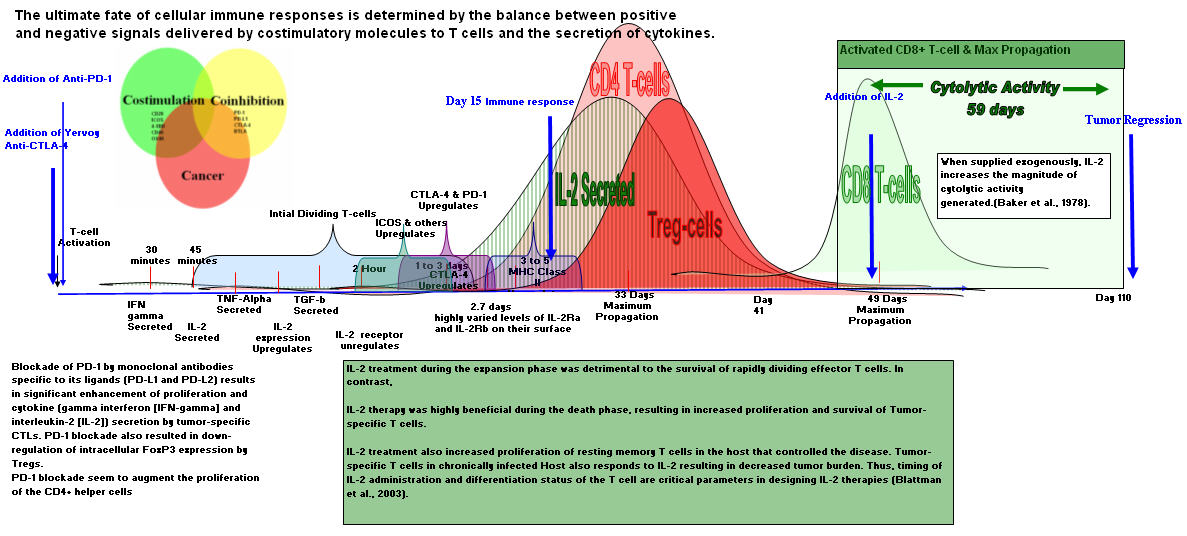
- October 12, 2011 at 9:28 pm
Harry,
Did you have inflammation 15 days after I was infused with Anti-CTLA-4?
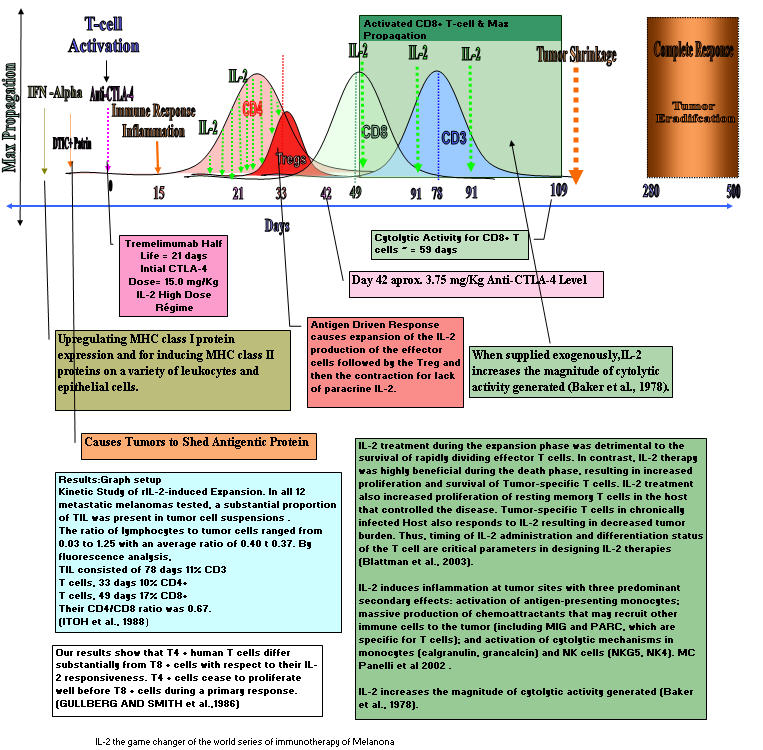
Well I did. It is a tell tale sign that I vaccinated myself with help of Anti-CTLA-4. Self vaccinated with my own Tumor-Specific Antigen. This very simular to Dr. Rosenburg's ACT therapy, but my was all in vivo. How long will it last, No one can say.
The graph is backed up with science.
for instance:
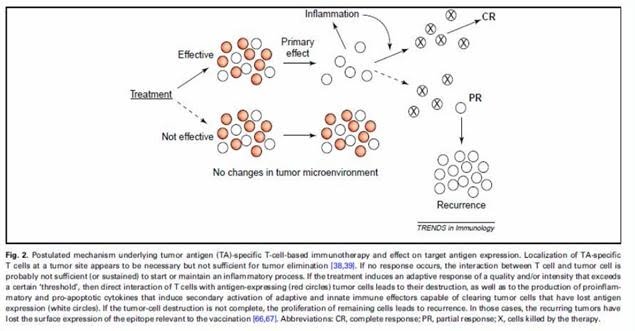
"Chemotherapy induces intratumoral expression of chemokines in cutaneous melanoma, favoring T cell infiltration and tumor control"
In conclusion, the present study identifies CXCR3 ligands and CCL5 as the main determinants of
T cell infiltration into cutaneous metastases and shows that chemotherapy, by inducing
expression of these chemokines within human tumors, may trigger T cell infiltration and tumor
control, resulting in prolonged patient survival. Therefore, screening for chemotherapeutic
products able to induce the expression of T cell attracting-chemokines in cancer cells may
identify drugs that improve the efficacy of immunotherapy
Corresponding author: Jean-Pierre Abastado, Laboratory of Tumour Immunology, Singapore
Immunology Network, 8A Biomedical Grove, #04-06 Immunos, Singapore 138648.
Tel: +65 6407 0003.
Fax: +65 6464 2057.
Email Dr. Abastado for a copy of his paper.
————————————————————————————————————-
Sensitization of a human ovarian cancer cell line to
temozolomide by simultaneous attenuation of the
Bcl-2 antiapoptotic protein and DNA repair by
O6-alkylguanine-DNA alkyltransferase
Introduction
"Temozolomide and or DTIC is an alkylating agent that mediates its cytotoxic effect by forming O6-methylguanine (O6-meG)DNA adducts, which during DNA replication pair preferentially with thymidine. These O6-meG:T mispairs can result in a G-to-A point mutation during a subsequent round of DNA replication but are also substrates for the postreplication mismatch repair pathway, which
fter a further round of DNA replication leads to apoptosis (1). O6-meG DNA adducts can be repaired by the DNA repair protein O6-alkylguanine-DNA alkyltransferase (MGMT), which removes adducts from the O6 position of guanine by accepting them onto a cysteine residue within its active site. Furthermore, fibroblasts and bone marrow cells of MGMT knockout mice are significantly more sensitive to the toxic effects of temozolomide than those from MGMT wild-type mice (2). The protective role of MGMT against the cytotoxic effect of temozolomide has been shown in human cell lines (3) and human xenograft models (4). MGMT can be inactivated by free guanine base derivatives that have alkyl groups at the O6 position, which act as pseudosubstrates.’’ O6-benzylguanine (5) and O6-(4-bromothenyl) guanine (PaTrin-2, Patrin, Lomeguatrib, KuDOS, Cambridge, United Kingdom; ref. 6) have been identified as the most promising MGMT inactivators. Compared with temozolomide used as a single agent, the combination
PaTrin-2-temozolomide has been shown to significantly increase tumor growth inhibition in human melanoma xenografts (7). "PaTrin-2 and O6-benzylguanine have recently entered phase I/II clinical trials.
DTIC+ Patrin-2 make the tumor cells more easily killed by Chemotherpy
I have spent the last 4 years collecting papers on this subject matter and piecing it together. You should see my hard drive. Paper/ powerpoints/ doctors email
I hope I can say I told you so in 10 to 20 years. Only time will tell.
I wish you well
-
- October 12, 2011 at 9:28 pm
Harry,
Did you have inflammation 15 days after I was infused with Anti-CTLA-4?
Well I did. It is a tell tale sign that I vaccinated myself with help of Anti-CTLA-4. Self vaccinated with my own Tumor-Specific Antigen. This very simular to Dr. Rosenburg's ACT therapy, but my was all in vivo. How long will it last, No one can say.
The graph is backed up with science.
for instance:
"Chemotherapy induces intratumoral expression of chemokines in cutaneous melanoma, favoring T cell infiltration and tumor control"
In conclusion, the present study identifies CXCR3 ligands and CCL5 as the main determinants of
T cell infiltration into cutaneous metastases and shows that chemotherapy, by inducing
expression of these chemokines within human tumors, may trigger T cell infiltration and tumor
control, resulting in prolonged patient survival. Therefore, screening for chemotherapeutic
products able to induce the expression of T cell attracting-chemokines in cancer cells may
identify drugs that improve the efficacy of immunotherapy
Corresponding author: Jean-Pierre Abastado, Laboratory of Tumour Immunology, Singapore
Immunology Network, 8A Biomedical Grove, #04-06 Immunos, Singapore 138648.
Tel: +65 6407 0003.
Fax: +65 6464 2057.
Email Dr. Abastado for a copy of his paper.
————————————————————————————————————-
Sensitization of a human ovarian cancer cell line to
temozolomide by simultaneous attenuation of the
Bcl-2 antiapoptotic protein and DNA repair by
O6-alkylguanine-DNA alkyltransferase
Introduction
"Temozolomide and or DTIC is an alkylating agent that mediates its cytotoxic effect by forming O6-methylguanine (O6-meG)DNA adducts, which during DNA replication pair preferentially with thymidine. These O6-meG:T mispairs can result in a G-to-A point mutation during a subsequent round of DNA replication but are also substrates for the postreplication mismatch repair pathway, which
fter a further round of DNA replication leads to apoptosis (1). O6-meG DNA adducts can be repaired by the DNA repair protein O6-alkylguanine-DNA alkyltransferase (MGMT), which removes adducts from the O6 position of guanine by accepting them onto a cysteine residue within its active site. Furthermore, fibroblasts and bone marrow cells of MGMT knockout mice are significantly more sensitive to the toxic effects of temozolomide than those from MGMT wild-type mice (2). The protective role of MGMT against the cytotoxic effect of temozolomide has been shown in human cell lines (3) and human xenograft models (4). MGMT can be inactivated by free guanine base derivatives that have alkyl groups at the O6 position, which act as pseudosubstrates.’’ O6-benzylguanine (5) and O6-(4-bromothenyl) guanine (PaTrin-2, Patrin, Lomeguatrib, KuDOS, Cambridge, United Kingdom; ref. 6) have been identified as the most promising MGMT inactivators. Compared with temozolomide used as a single agent, the combination
PaTrin-2-temozolomide has been shown to significantly increase tumor growth inhibition in human melanoma xenografts (7). "PaTrin-2 and O6-benzylguanine have recently entered phase I/II clinical trials.
DTIC+ Patrin-2 make the tumor cells more easily killed by Chemotherpy
I have spent the last 4 years collecting papers on this subject matter and piecing it together. You should see my hard drive. Paper/ powerpoints/ doctors email
I hope I can say I told you so in 10 to 20 years. Only time will tell.
I wish you well
-
- October 12, 2011 at 9:46 pm
I'm impressed by your enthusiasm and dedication. As you say, "only time will tell" if all your theories are borne out as scientific facts. I'm paying people to check all this stuff out, but they work for the government – so I'm not expecting much of anything very soon!
Best wishes,
Harry
-
- October 12, 2011 at 9:46 pm
I'm impressed by your enthusiasm and dedication. As you say, "only time will tell" if all your theories are borne out as scientific facts. I'm paying people to check all this stuff out, but they work for the government – so I'm not expecting much of anything very soon!
Best wishes,
Harry
-
- October 12, 2011 at 9:46 pm
I'm impressed by your enthusiasm and dedication. As you say, "only time will tell" if all your theories are borne out as scientific facts. I'm paying people to check all this stuff out, but they work for the government – so I'm not expecting much of anything very soon!
Best wishes,
Harry
-
- October 12, 2011 at 9:28 pm
Harry,
Did you have inflammation 15 days after I was infused with Anti-CTLA-4?
Well I did. It is a tell tale sign that I vaccinated myself with help of Anti-CTLA-4. Self vaccinated with my own Tumor-Specific Antigen. This very simular to Dr. Rosenburg's ACT therapy, but my was all in vivo. How long will it last, No one can say.
The graph is backed up with science.
for instance:
"Chemotherapy induces intratumoral expression of chemokines in cutaneous melanoma, favoring T cell infiltration and tumor control"
In conclusion, the present study identifies CXCR3 ligands and CCL5 as the main determinants of
T cell infiltration into cutaneous metastases and shows that chemotherapy, by inducing
expression of these chemokines within human tumors, may trigger T cell infiltration and tumor
control, resulting in prolonged patient survival. Therefore, screening for chemotherapeutic
products able to induce the expression of T cell attracting-chemokines in cancer cells may
identify drugs that improve the efficacy of immunotherapy
Corresponding author: Jean-Pierre Abastado, Laboratory of Tumour Immunology, Singapore
Immunology Network, 8A Biomedical Grove, #04-06 Immunos, Singapore 138648.
Tel: +65 6407 0003.
Fax: +65 6464 2057.
Email Dr. Abastado for a copy of his paper.
————————————————————————————————————-
Sensitization of a human ovarian cancer cell line to
temozolomide by simultaneous attenuation of the
Bcl-2 antiapoptotic protein and DNA repair by
O6-alkylguanine-DNA alkyltransferase
Introduction
"Temozolomide and or DTIC is an alkylating agent that mediates its cytotoxic effect by forming O6-methylguanine (O6-meG)DNA adducts, which during DNA replication pair preferentially with thymidine. These O6-meG:T mispairs can result in a G-to-A point mutation during a subsequent round of DNA replication but are also substrates for the postreplication mismatch repair pathway, which
fter a further round of DNA replication leads to apoptosis (1). O6-meG DNA adducts can be repaired by the DNA repair protein O6-alkylguanine-DNA alkyltransferase (MGMT), which removes adducts from the O6 position of guanine by accepting them onto a cysteine residue within its active site. Furthermore, fibroblasts and bone marrow cells of MGMT knockout mice are significantly more sensitive to the toxic effects of temozolomide than those from MGMT wild-type mice (2). The protective role of MGMT against the cytotoxic effect of temozolomide has been shown in human cell lines (3) and human xenograft models (4). MGMT can be inactivated by free guanine base derivatives that have alkyl groups at the O6 position, which act as pseudosubstrates.’’ O6-benzylguanine (5) and O6-(4-bromothenyl) guanine (PaTrin-2, Patrin, Lomeguatrib, KuDOS, Cambridge, United Kingdom; ref. 6) have been identified as the most promising MGMT inactivators. Compared with temozolomide used as a single agent, the combination
PaTrin-2-temozolomide has been shown to significantly increase tumor growth inhibition in human melanoma xenografts (7). "PaTrin-2 and O6-benzylguanine have recently entered phase I/II clinical trials.
DTIC+ Patrin-2 make the tumor cells more easily killed by Chemotherpy
I have spent the last 4 years collecting papers on this subject matter and piecing it together. You should see my hard drive. Paper/ powerpoints/ doctors email
I hope I can say I told you so in 10 to 20 years. Only time will tell.
I wish you well
-
- October 12, 2011 at 8:22 pm
Jim, I don't want to pick an argument with you – most of the treatments you champion are doubtlessly on the right path. But as elegantly as you present your information (and you have wonderful graphics), you are not living proof that your regimen is the "magic bullet." Nor are the other NED patients that you allude to. Your individual health outcome is anecdotal information, not scientific proof.
I have learned the hard way not to tempt the NED gods. After being almost 11 years NED after lung metastisis, I thought I was done with this thing. I even thought that the immunological trials I went through (vaccine and leukine) may have been the nails in the coffin. Imagine my surprise when the beast woke up and bit me this year!
Best wishes,
Harry
-
- October 12, 2011 at 7:18 pm
Harry, I want tell you, YOU have heard it here first.
I am living proof. From Stage IV to NED without surgery of 40 + Lung nodules in both lobes and sub Q's. Also there are others that had a simular regime, NED also. All the science is not worked out, but the theory is there. Sequence and Timing is the name of the game.
Warm regards,
Jimmy B
-
- October 12, 2011 at 6:55 pm
I really hope the "1-2-3" path you outline indeed leads to that holy grail, the "magic bullet." We must keep in mind the long, sometimes insurmountable, path between the theoretical and the eventual actual. But we can always hope – and be thankful for the advances of the last few years, even though they aren't all that we want.
Best wishes,
Harry
-
- October 12, 2011 at 6:55 pm
I really hope the "1-2-3" path you outline indeed leads to that holy grail, the "magic bullet." We must keep in mind the long, sometimes insurmountable, path between the theoretical and the eventual actual. But we can always hope – and be thankful for the advances of the last few years, even though they aren't all that we want.
Best wishes,
Harry
-
- October 12, 2011 at 6:03 pm
Harry, I thinks the "Magic Bullet" will be a combinatorial therapy. It will most likely drugs strung in a sequence that :
1) A drug combo to make the tumor more susceptible to Chemo to shed Tumor-Specific antigens from dying tumor cells (DTIC,Patrin-2,Cisplatin,TMZ,radiation,biochemo..etc)
2) a drug combo to suppress the Tregs and help activate T-cells (Yervoy,Anti-PD-1, Anti-Gal-3 ..etc)
3) Finally a drug that keeps the T-cell (Cytotoxic T-lymphocytes) activated, functional and that is needed for survival.
-
- October 12, 2011 at 6:03 pm
Harry, I thinks the "Magic Bullet" will be a combinatorial therapy. It will most likely drugs strung in a sequence that :
1) A drug combo to make the tumor more susceptible to Chemo to shed Tumor-Specific antigens from dying tumor cells (DTIC,Patrin-2,Cisplatin,TMZ,radiation,biochemo..etc)
2) a drug combo to suppress the Tregs and help activate T-cells (Yervoy,Anti-PD-1, Anti-Gal-3 ..etc)
3) Finally a drug that keeps the T-cell (Cytotoxic T-lymphocytes) activated, functional and that is needed for survival.
-
- October 12, 2011 at 3:47 pm
Jim,
Interesting that you should post the research done by Dr. Lo at UCLA. My Onc is Dr. Ribas at UCLA who has been doing the research studies with Dr. Lo. on Braf.
Long story short, I had an appt. with Dr. Ribas last week. Dr. Ribas told me, based on their most recent research, Dr. Lo & himself believe that even with combining Braf with "combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways" that tumors will still eventually become resistant to the Braf/combo drugs.It would only be a matter of time.
When discussing if I should do the Braf/Mek combo trial, he recommended that I do an immmnunolgy drug like IPI or a PD1 drug. Dr. Ribas told me based on their most recent research that when you take an inhibitor drug, somehow the inhibitor drug alters the tumor. Then when the Braf/combo eventually stops working, because the tumor has been altered and there is tumor progresses, Dr.Ribas says it is then more difficult for a person's immune system to kill the tumor cells.
Needless to say, it was disappointing to hear that the Braf/ combo drugs were not going to be the magic bullet.
For what it is worth, I am taking Dr.Ribas advice and doing an immmunology treatment.
-
- October 12, 2011 at 1:23 pm
"Ultimately, the research suggested that a combination of drugs blocking the PI3K, mTORC1/2 and MEK1/2 pathways represent the optimal combination for use with a BRAF inhibitor to mitigate the development of resistance. "
"All three compounds we used to overcome resistance to BRAF inhibition are already undergoing clinical evaluation. Therefore, we believe this particular combination approach represents a promising and translatable strategy for addressing BRAF inhibitor resistance in a subset of melanomas," Dr. Lo says.
"Among clinical trials currently enrolling melanoma patients with BRAF mutations are those combining BRAF and MEK inhibition and others combining PI3K/mTOR and MEK inhibition. Other highly-watched trials include those which combine a BRAF inhibitor with ipilimumab. "
Source: Dematology Times
- You must be logged in to reply to this topic.